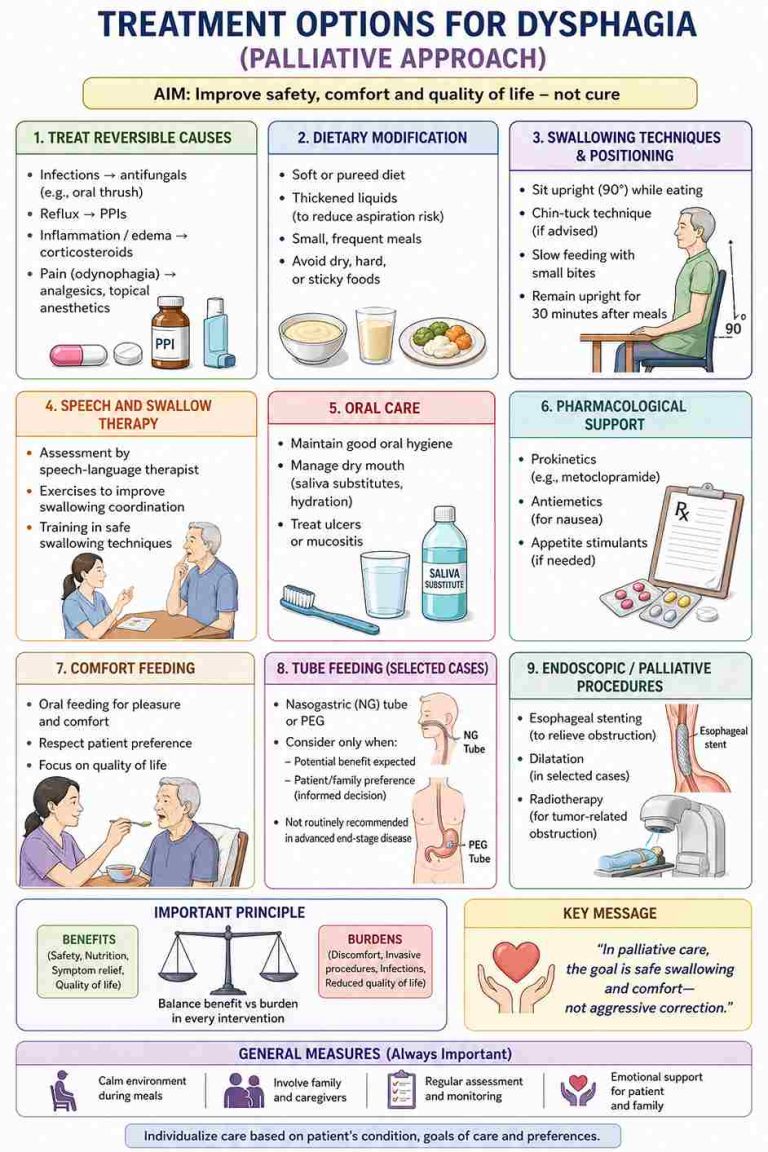
Dysphagia (difficulty swallowing) is common in advanced illnesses such as stroke, neurodegenerative disorders, and advanced cancer. It can lead to aspiration, malnutrition, dehydration, and significant distress for both patients and caregivers. In palliative care, the focus shifts from aggressive nutritional correction to comfort, dignity, and patient-centered decision-making.
A key clinical dilemma is choosing between comfort feeding (oral feeding for pleasure and comfort) and tube feeding (enteral nutrition). This decision requires careful consideration of the patient’s condition, prognosis, goals of care, and potential benefits versus burdens.
What is Dysphagia?
Dysphagia is an impairment in the ability to swallow food or liquids safely. It may present as:
Dysphagia has a significant impact on patients, particularly in advanced illness, affecting both physical health and overall quality of life. Difficulty in swallowing can lead to malnutrition, dehydration, and weight loss, as patients are unable or unwilling to eat adequately. It also increases the risk of aspiration, which may result in recurrent chest infections or aspiration pneumonia. Beyond physical complications, dysphagia can cause considerable psychological distress, including fear of choking, anxiety during meals, and loss of the pleasure associated with eating. Patients may begin to avoid food, leading to social isolation, as meals are often an important part of family interaction. In palliative care, these effects can further contribute to fatigue, weakness, and reduced functional status, making dysphagia a major factor influencing both patient comfort and caregiver burden.
Dysphagia in advanced illness presents a complex clinical and ethical challenge, particularly when deciding between comfort feeding and tube feeding. This decision is not purely medical—it is deeply influenced by patient goals, prognosis, quality of life, and family expectations.
In palliative care, dysphagia often reflects disease progression, especially in conditions such as advanced cancer, neurodegenerative disorders, or frailty. While tube feeding may appear to offer a solution for maintaining nutrition, evidence suggests that in many advanced cases, it does not significantly improve survival, prevent aspiration, or enhance quality of life. In fact, it may introduce additional burdens such as discomfort, infections, need for restraints, and reduced social interaction during meals.
On the other hand, comfort feeding focuses on allowing the patient to eat and drink for pleasure and comfort, even if intake is minimal. This approach prioritizes dignity, autonomy, and the emotional value of eating, which is often deeply meaningful for patients and families. Although there is a risk of aspiration, careful techniques such as upright positioning, slow feeding, and texture modification can help reduce complications while maintaining quality of life.
A key aspect of management is communication and shared decision-making. Families may struggle with the idea of reduced intake and often equate feeding with care and survival. It is essential for healthcare providers to educate and reassure caregivers that decreased eating is a natural part of advanced illness and not necessarily a sign of suffering. Discussing goals of care early, including advance directives, can help align treatment decisions with patient preference.
Ultimately, the choice between comfort feeding and tube feeding should be individualized, balancing potential benefits and burdens. In most end-stage situations, comfort feeding is preferred, as it aligns with the fundamental principles of palliative care—relief of suffering, preservation of dignity, and enhancement of quality of life.
|
Aspect
|
Comfort Feeding (Oral, Risk-Accepting)
|
Tube Feeding (NG / PEG / PEJ)
|
|---|---|---|
|
Primary goal
|
Comfort, pleasure, dignity
|
Nutritional delivery
|
|
Core philosophy
|
Quality of life over intake
|
Maintain/augment intake
|
|
Invasive
|
Non-invasive
|
Invasive (tube placement)
|
|
Patient experience
|
Enjoys taste, social meals, autonomy
|
Loss of taste/meal experience; device burden
|
|
Aspiration risk
|
Present; can be reduced with techniques
|
Not eliminated (aspiration of secretions/reflux still occurs)
|
|
Effect on survival
|
No clear reduction
|
Generally no meaningful survival benefit in end-stage disease
|
|
Complications
|
Choking, aspiration (manageable with precautions)
|
Tube dislodgement, infection, sinusitis (NG), site issues (PEG), diarrhoea, reflux
|
|
Caregiver burden
|
Supervised feeding; emotionally meaningful
|
Technical care (feeds, pumps, site care), training required
|
|
Cost
|
Low
|
Higher (procedure + equipment + supplies)
|
|
Ethical alignment
|
Strong with autonomy & dignity
|
Depends on goals; risk of non-beneficial treatment
|
|
Typical indications
|
Advanced disease, poor prognosis, patient preference for oral intake
|
Reversible conditions, short-term support, clear patient preference for artificial feeding
|
|
End-of-life use
|
Preferred approach
|
Generally, not recommended unless specific indication
|
Takeaways

I am a physician specialized in Palliative Medicine (MD) with a strong commitment to improving the quality of life for patients with life-limiting illnesses. My clinical focus is on comprehensive symptom management, holistic patient care, and psychosocial support for patients and families.Beyond clinical practice, I am deeply interested in palliative care education, research, and integrating evidence-based practices into patient-centered care. I aim to contribute to the growth of palliative care services, raise awareness about end-of-life issues, and advocate for a more compassionate healthcare system.