Nutrition in Palliative Care: Managing Cachexia and Loss of Appetite
Introduction
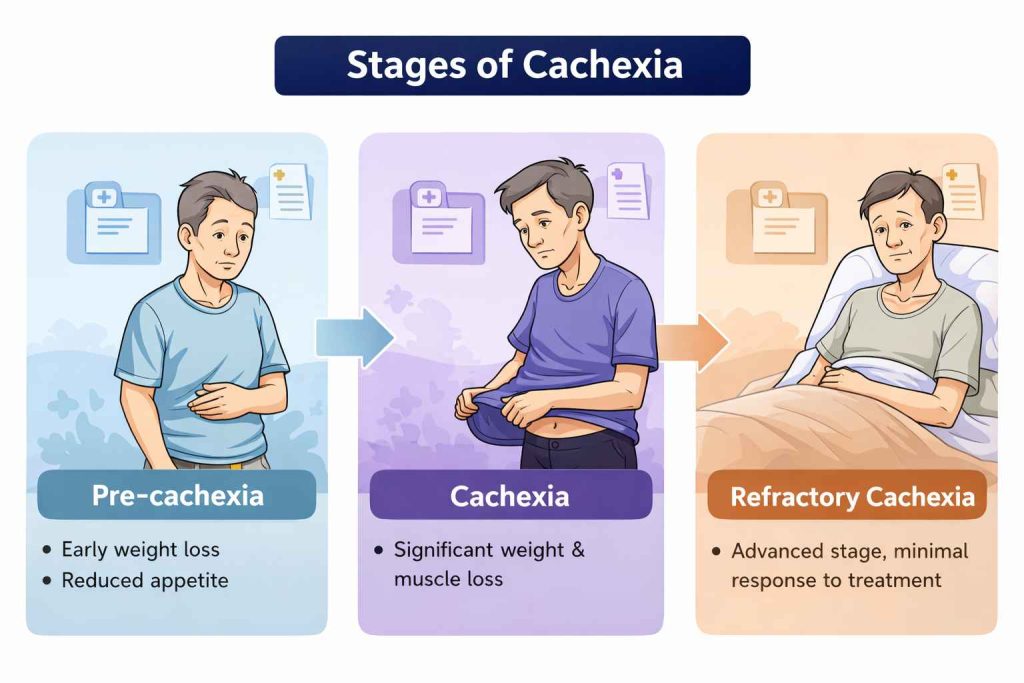
Malnutrition is a common and challenging problem in patients with advanced illness, particularly in those with cancer. Many patients experience cachexia, a complex metabolic syndrome characterized by involuntary weight loss, muscle wasting, reduced appetite, and functional decline. Unlike simple starvation, cachexia is driven by underlying disease processes and is often resistant to conventional nutritional support.
Loss of appetite (anorexia) further compounds the problem, leading to decreased oral intake, weakness, fatigue, and reduced quality of life. These changes can be distressing not only for patients but also for caregivers, who often equate eating with recovery and well-being.
In palliative care, the focus shifts from aggressive nutritional correction to a comfort-oriented, patient-centered approach. The goal is not to reverse cachexia completely, but to maximize comfort, maintain strength as much as possible, and respect patient preferences. Gentle nutritional support, symptom control, and emotional reassurance play a crucial role in managing these patients.
What is Cachexia? – Cachexia is a complex metabolic syndrome seen in patients with advanced illness, especially cancer. It is characterized by ongoing loss of weight, particularly muscle mass, which cannot be fully reversed by normal nutritional intake.
Cachexia develops due to a combination of:
Anorexia–Cachexia Syndrome (ACS) is a multifactorial condition seen in advanced illness, especially cancer, characterized by:
- Loss of appetite (anorexia)
- Progressive weight loss
- Muscle wasting (cachexia)
- Fatigue and functional decline
Cachexia vs Starvation – Both are different
How Anorexia Affects Patients and Families
Management of Anorexia–Cachexia Syndrome (ACS) in Palliative Care
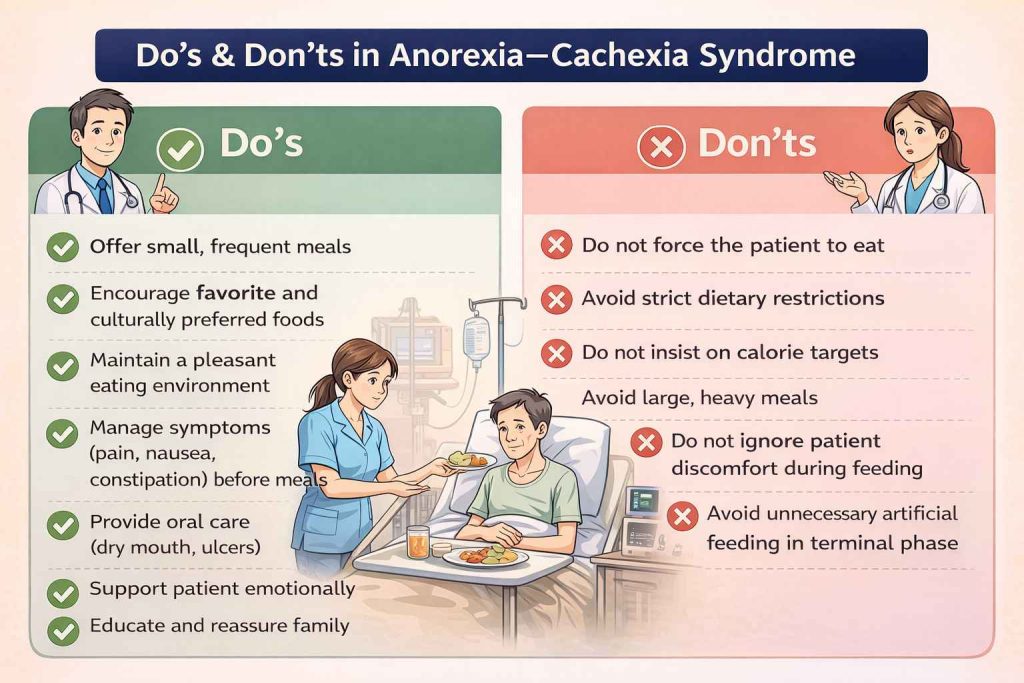
Principles of Management
- Focus on comfort, not weight gain
- Individualize treatment based on patient condition
- Avoid force feeding
- Respect patient preferences
- Provide family counseling and reassurance
Nutritional Strategies
- Offer small, frequent meals
- Use high-calorie, high-protein foods
- Encourage favorite foods (no strict diet rules)
- Provide nutritional supplements if tolerated
- Use soft or liquid diet if chewing/swallowing is difficult
Goal: Pleasure and comfort in eating
Management of Reversible Causes - treat the reversible cause of anorexia if any, such as nausea, vomiting, constipation, diarrhoea, pain, dryness of mouth, oral ulcer, mucositis accordingly
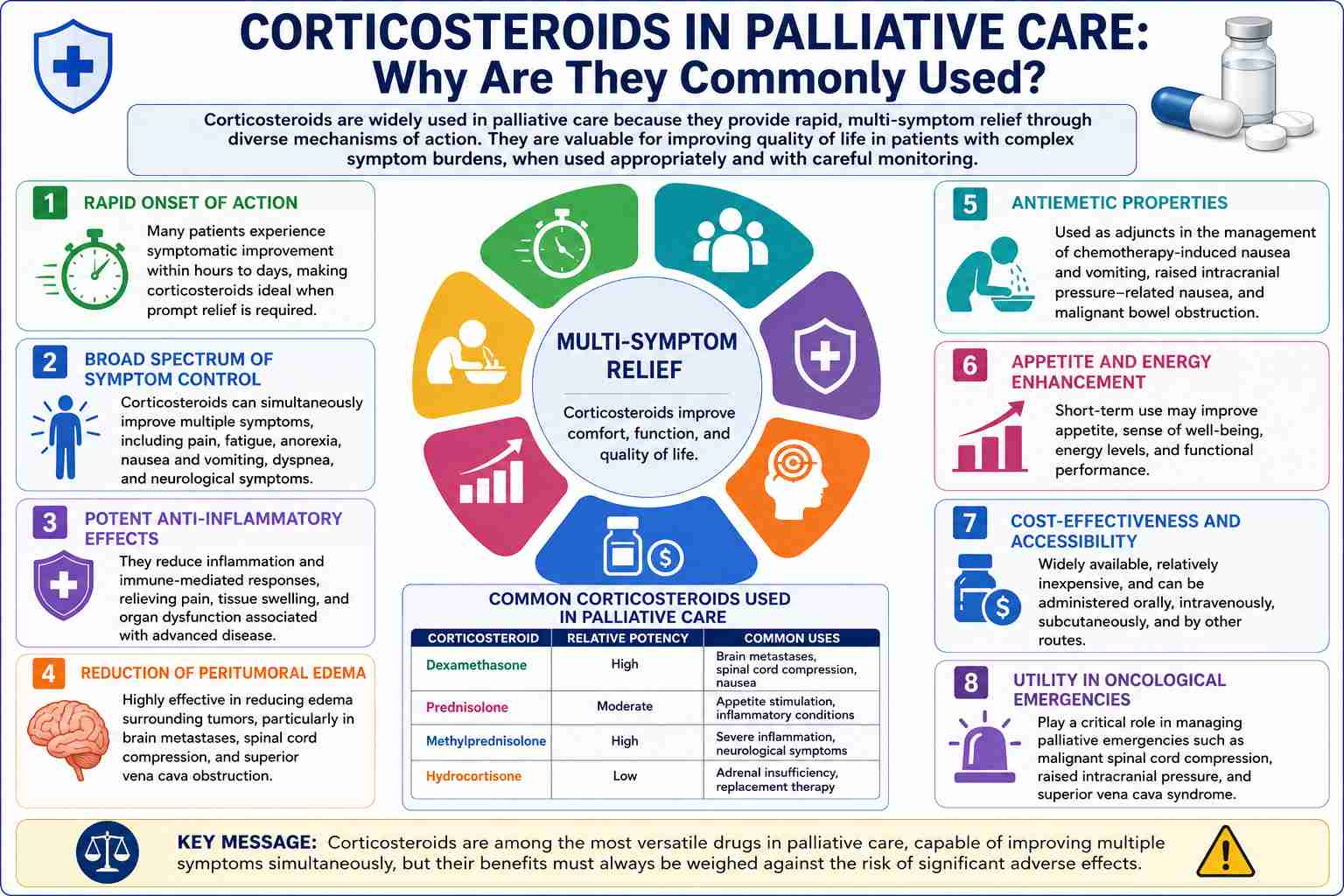
Pharmacological Management
Non-Pharmacological Management
- Improve meal environment (pleasant, relaxed)
- Encourage family involvement
- Avoid pressure to eat
- Provide emotional reassurance
Family Counselling
- Explain that loss of appetite is part of disease process
- Reassure: “Not eating does not mean suffering”
Anorexia–Cachexia Syndrome is not just a nutritional problem—it is a disease-driven process requiring holistic palliative care.