Respiratory tract secretions are a common occurrence during the final days and hours of life and may lead to the characteristic sound known as the “death rattle.” This phenomenon results from the accumulation of saliva and bronchial secretions in patients who have lost the ability to swallow or clear secretions effectively. Although these secretions are often not distressing to the unconscious patient, they can be highly distressing for family members and caregivers.
Management of terminal secretions involves a combination of non-pharmacological and pharmacological interventions. Among pharmacological options, anticholinergic drugs are the most commonly used agents because they reduce the production of new secretions by blocking muscarinic receptors within salivary and respiratory glands. However, these medications differ considerably in their pharmacokinetic properties, including onset of action, duration of effect, blood-brain barrier penetration, and route of administration.
Understanding the pharmacokinetics of anticholinergic agents is essential for selecting the most appropriate drug in different end-of-life situations. Appropriate use can improve symptom control, reduce caregiver distress, and enhance the quality of end-of-life care while minimizing adverse effects such as delirium, urinary retention, and excessive drying of mucosal surfaces.
Patients may complain of:
The patient often does not express distress verbally. Instead, clinicians and family members observe:
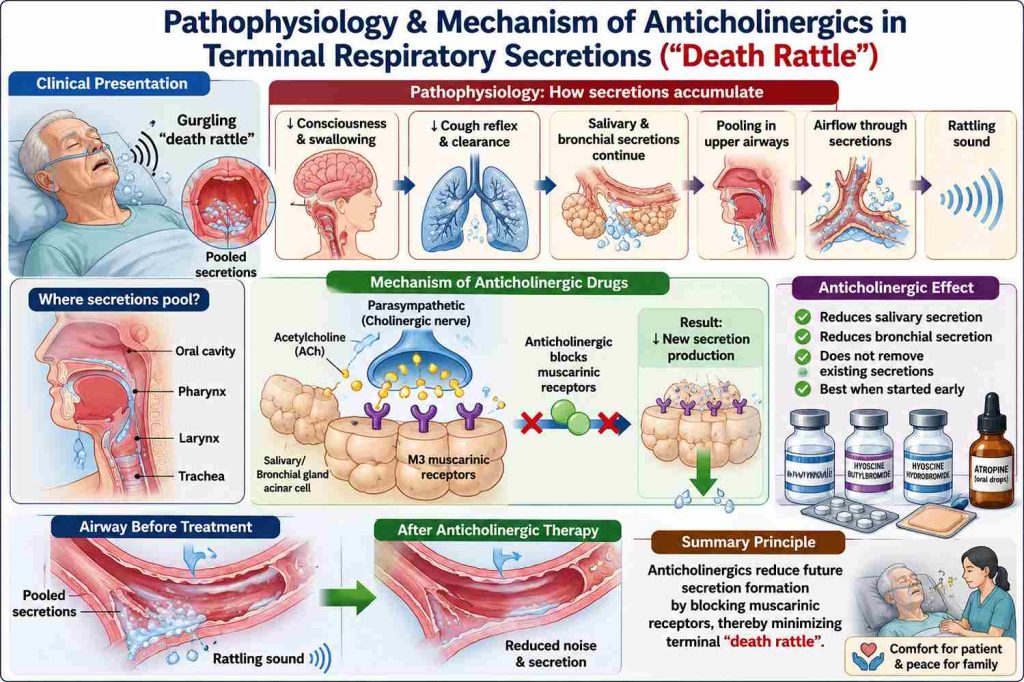
Terminal respiratory secretions, occur when patients are in the final stages of life lose the ability to effectively swallow, cough, or clear normal oral and bronchial secretions. As consciousness decreases and neuromuscular function deteriorates, secretions accumulate in the oropharynx and upper airways. Air moving through these pooled secretions produces the characteristic gurgling or rattling sound heard during breathing. Importantly, the sound does not necessarily indicate respiratory distress, and many unconscious patients are believed to be unaware of it. However, it can be distressing for family members and healthcare providers.
Although anticholinergic drugs share a common mechanism of reducing salivary and bronchial secretions through muscarinic receptor blockade, they differ significantly in their pharmacokinetic properties. Factors such as onset of action, duration of effect, route of administration, lipid solubility, and ability to cross the blood-brain barrier influence both their clinical effectiveness and adverse-effect profile. Understanding these differences helps clinicians select the most appropriate agent for secretion management at the end of life.
|
Drug
|
Onset Of Action
|
Duration
|
BBB Penetration
|
Major Advantage
|
Major Limitation
|
|---|---|---|---|---|---|
|
Glycopyrrolate
|
15–30 min
|
6–8 h
|
Minimal
|
Less delirium and sedation
|
May require repeated dosing
|
|
Hyoscine Butylbromide
|
30 min
|
4–6 h
|
Minimal
|
Widely used in palliative care
|
Short duration
|
|
Hyoscine Hydrobromide (Scopolamine)
|
30–60 min
|
Up to 72 h (patch)
|
Significant
|
Long duration
|
Delirium, confusion
|
|
Atropine
|
15–30 min
|
4–6 h
|
Significant
|
Easily administered (sublingual drops)
|
CNS adverse effects
|
Myth – “The strongest anticholinergic is always the best choice.”
Reality – The best choice depends on:

I am a physician specialized in Palliative Medicine (MD) with a strong commitment to improving the quality of life for patients with life-limiting illnesses. My clinical focus is on comprehensive symptom management, holistic patient care, and psychosocial support for patients and families.Beyond clinical practice, I am deeply interested in palliative care education, research, and integrating evidence-based practices into patient-centered care. I aim to contribute to the growth of palliative care services, raise awareness about end-of-life issues, and advocate for a more compassionate healthcare system.